LARYNGECTOMY.NET
Anatomical, functional and psychosocial consequences
Anatomical and functional consequences:
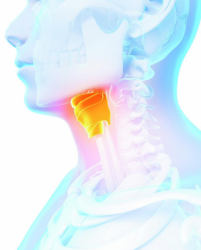
The three functions of the larynx, which are breathing, deglutition and speech will be directly affected by the surgery. The main impact of the surgery is a definitive separation of the digestive and respiratory tracts: the aerodigestive crossroads are no longer present.
Aerodigestive tracts prior to laryngectomy:

Aerodigestive tracts after laryngectomy:

Breathing is the main function of the larynx. Following total laryngectomy, the trachea is directly connected to the skin, at the level of the tracheostoma. Therefore, breathing takes place directly through this orifice.
Physiological breathing:
Breathing after total laryngectomy:
After surgery, the oral cavity and the nasal cavities no longer communicated with the neo-pharynx. Therefore there is no risk of food choking. Swallowing is preserved, thanks to the propulsion by the base of the tongue and the constrictor muscles of the pharynx.
Physiological swallowing:
Swallowing after total laryngectomy:
Finally, physiological speech, by vibration of vocal chords is definitively lost. New speech techniques will be taught to the patient during speech therapy sessions. In the presence of a phonatory prosthesis, the objective of speech re-education will be to develop a tracheo-oesophageal voice. In the absence of this prosthesis, the use of the oro-oesophageal voice will be taught to the patient.
Physiological speech:
Oro-oesophageal voice:
Tracheo-oesophageal voice (phonatory prosthesis):
Psychosocial consequences
The apparent sequels of the surgery are also important, with a major psychological impact. The presence of the tracheostoma in a visible zone, in the middle of the neck, in addition to the considerable modification of the voice, are two factors that strongly disturb the self-image, and undermine the communication and coping skills of the patient.
The life of the patient will thus be modified in different aspects. First of all, self-image and self-esteem will be profoundly modified. This could have a major effect on the mood of the patient and sometimes cause a depressive syndrome. Then, in public sphere, the patient could experience a lack of self-confidence and experience a self-withdrawal. In the intimate and private sphere, the loss of the voice and the presence of the tracheostoma could also lead to a lack of communication. Furthermore, the impact and the sequels of the surgery are not limited to the patient, but also affect the patient’s family in their daily life.
Therefore, it would seem essential that the patient be able to benefit from a psychological follow-up, in order to face these difficulties, improve his/her experience of the disease and his/her quality of life.
