LARYNGECTOMY.NET
Anatomical and functional changes
A total laryngectomy, which consists in removing the larynx, generates functional and anatomical changes. Explain to your patient his/her breathing and laryngeal voice functioned before the surgery, so that he/she can understand better how it will function afterwards. You may use diagrams to help you with this, as they are more easily understandable by your patient.
The larynx is at the crossroads of 3 functions; breathing, speech and swallowing, which will be modified following the surgery.
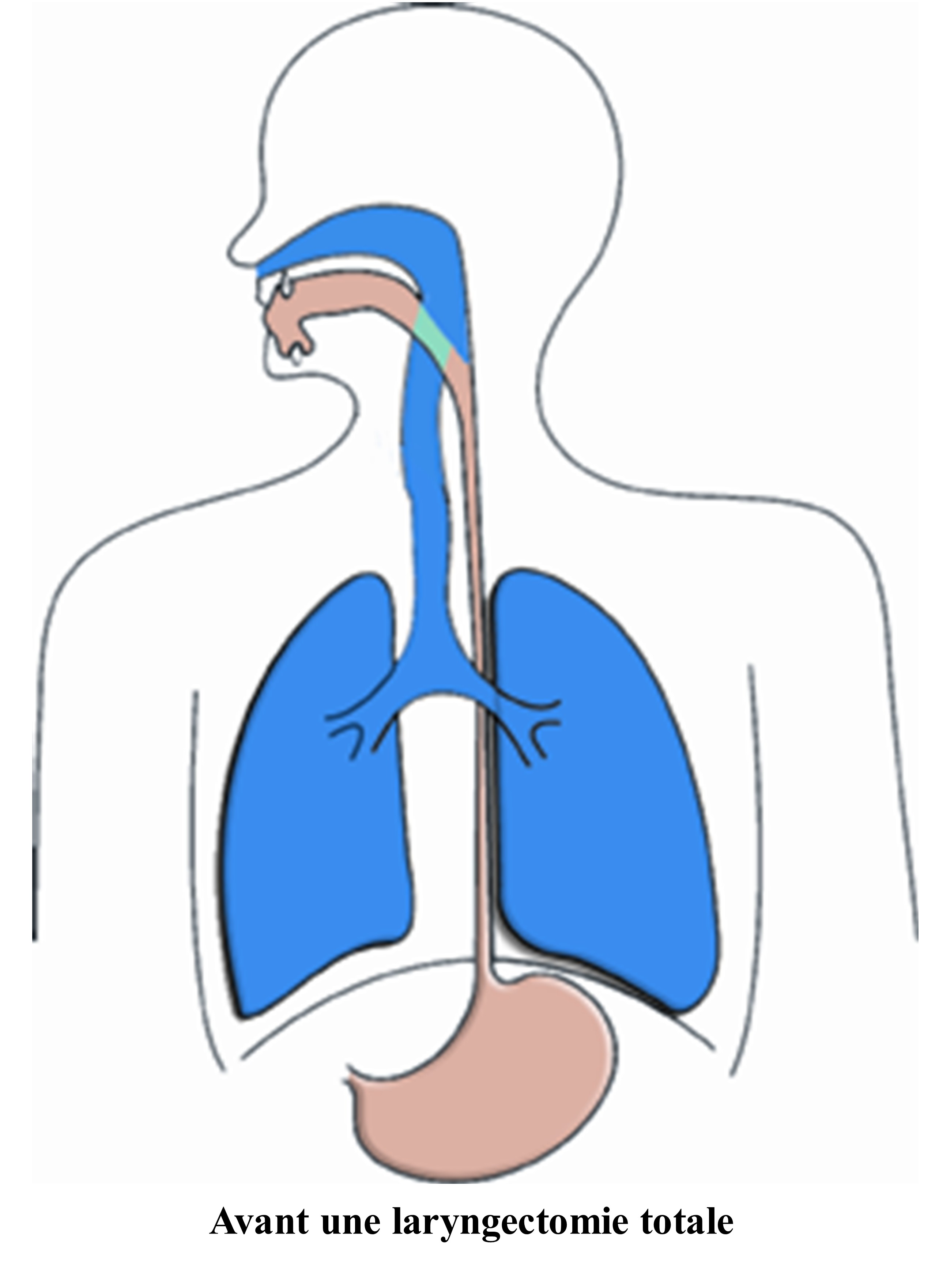
Before surgery, to:
– Breath: we inhale through the mouth and the nose. The air passes, when the vocal chords are relaxed and the larynx is open, through to go towards the lungs.
– Speak: on exhaling the larynx muscles contract and the vocal chords vibrate. The sound produced is modulated and enriched by the pharyngeal-oro-nasal cavity.
– Swallowing: (food, saliva or drink) the larynx rises and epiglottis tilts backwards preventing the food to enter into the trachea and then into the lungs. Therefore, food goes down the oesophagus and then into the stomach.
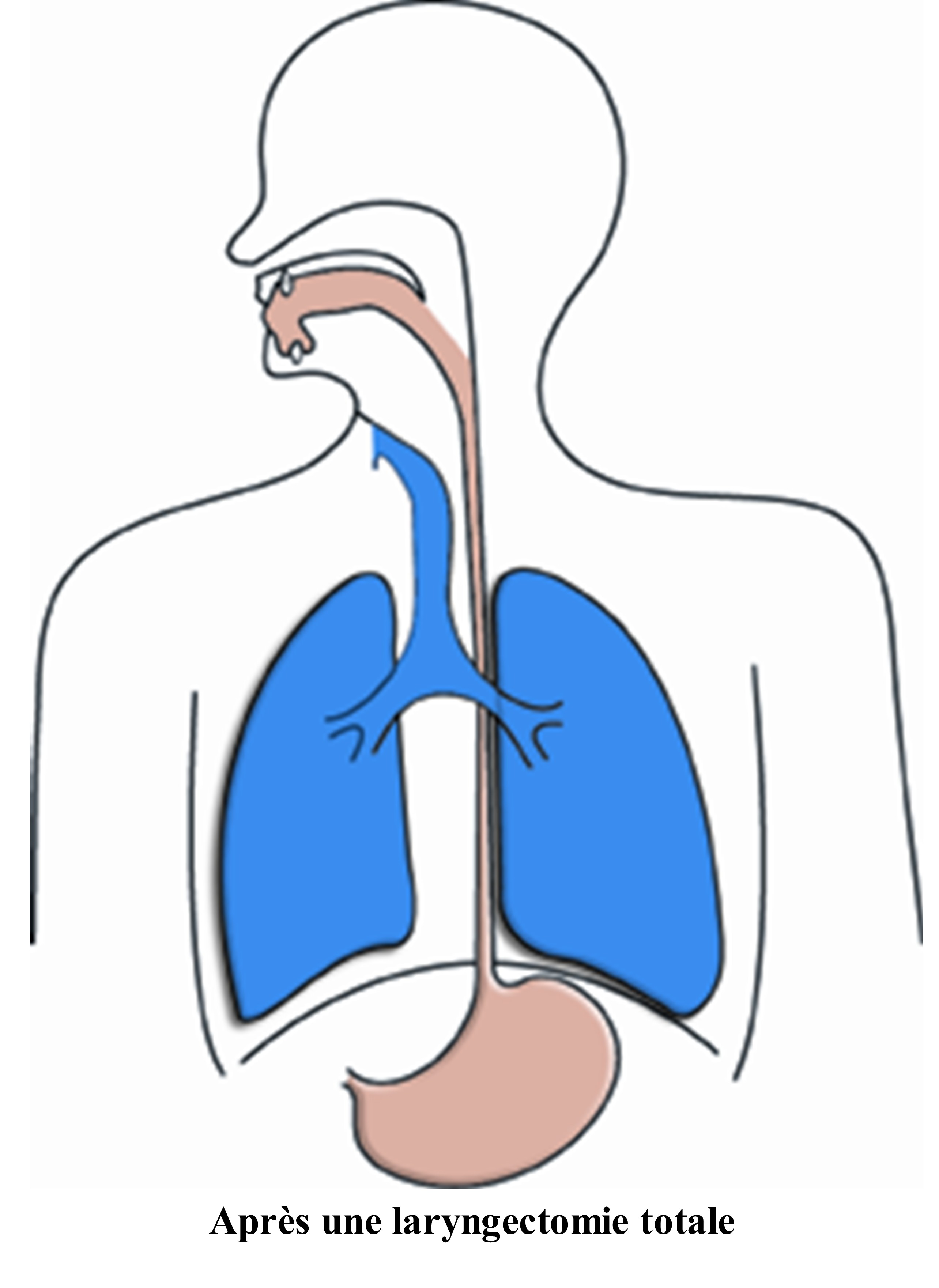
After surgery, breathing, speaking and swallowing will no longer take place in the same manner:
– Changes in terms of breathing:
– The air path is no longer the same. The air inhaled enters directly through the tracheostoma because the trachea has been attached to the front of the neck.
– The nose and the mouth can no longer carry out their air humidification, warming and filter roles. To compensate these functions, tracheal protections are proposed to the patients.
– Blocking breathing is now impossible therefore, physical efforts are more difficult. (WC, heavy loads, sports, etc.). Shortness of breath is often more significant.
– The loss of the sense of smell is a definitive consequence of the operation. However, there are techniques to recover the sense of smell that you can teach the patient during a session.
– With respect to the voice:
– When the surgeon removes the larynx, the vocal chords are also removed, therefore, the patient can no longer make sounds.
– Initially, the patient will have to write and use gestures and facial expressions to be understood. He/she can also whisper.
– Once the wound healing is complete the patient will be prescribed speech re-education to learn to use a substitution voice. This voice will not resemble his/her old laryngeal voice.
– With respect to the swallowing:
– Approximately 10 days after the surgery (depending on the healing) eating through the mouth will be possible again. Before these 10 days, the patient will be fed through a nasogastric tube.
– Approximately 10 days after the surgery (depending on the healing) eating through the mouth will be possible again. Before these 10 days, the patient will be fed through a nasogastric tube.
– Food choking will now become impossible.
– The reduction or loss of the sense of taste could be caused by the surgery and additional treatments.
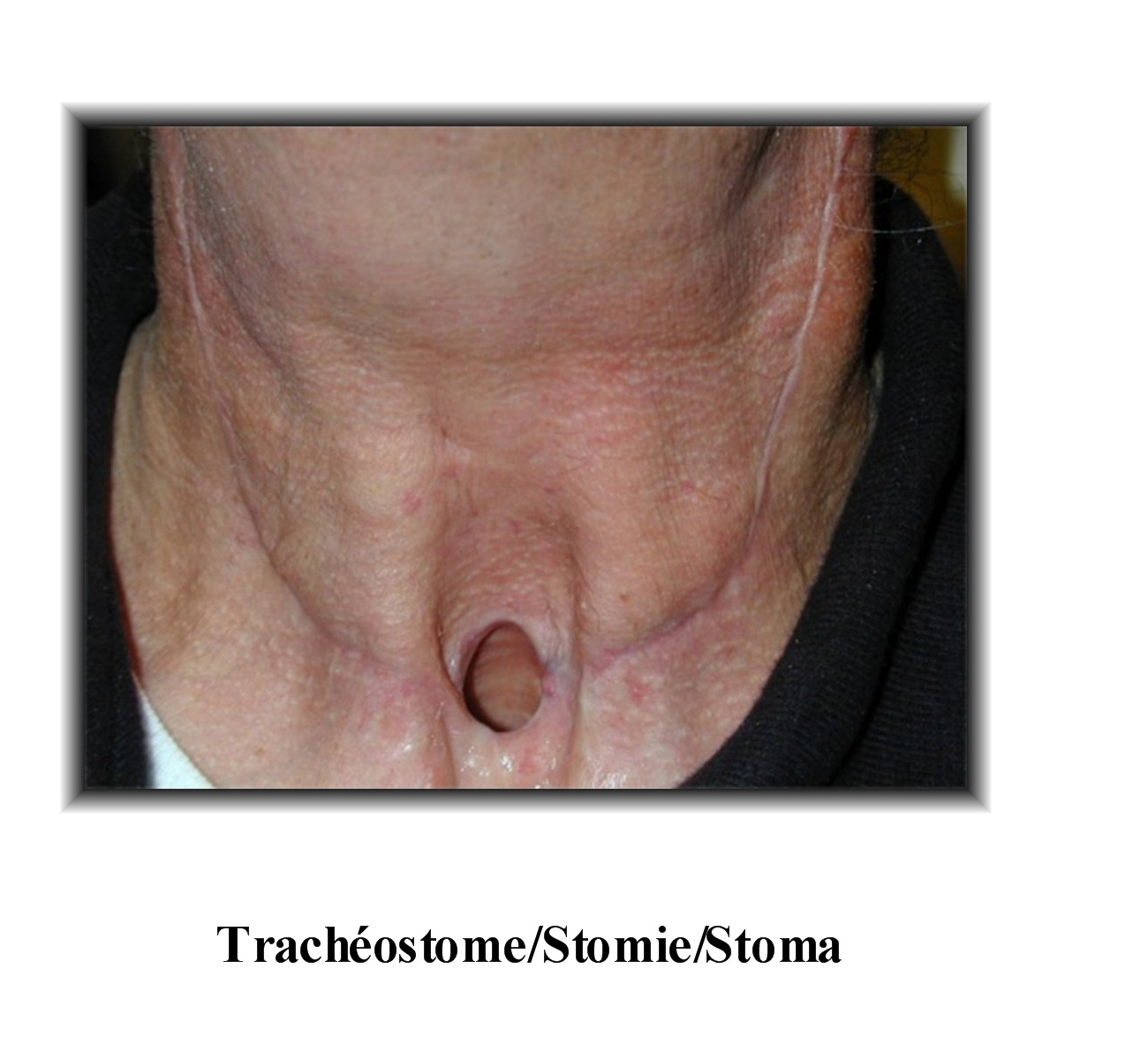
Once the larynx has been removed, the trachea will be connected to the front of the neck through a definitive opening. This opening is called a tracheostoma (also called “stoma”).